

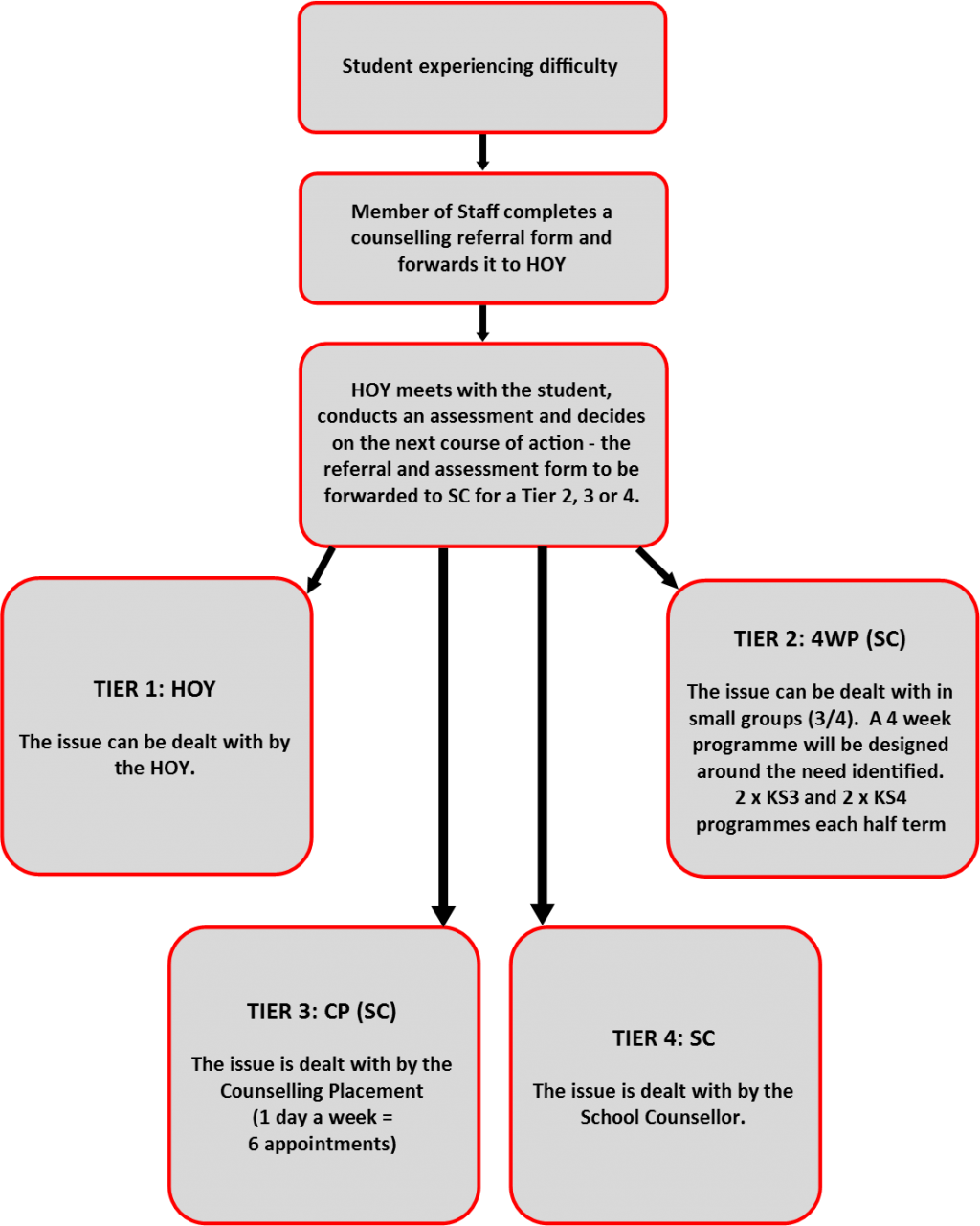
Counselling Referral Process and Referral Form
COUNSELLING REFERRAL FORM
| Requested by: | Date: | ||
| Students’ Name: | |||
| Tutor Group: | Urgency of referral: | (1 low – 10 high) |
Please give as much information as possible as this will speed up the referral process.
- What is your cause for concern?
- Please give any relevant information about the student’s background or significant life events
- How is the student functioning in school (academically, socially and behaviour)?
- Have you discussed the possibility of counselling with the student? What was their reaction?
- Are the students’ parents aware of this approach? What was their reaction?
- Are you aware of other professional involvement with this student? (i.e. Social Services, CAMHS, GP, etc.)
Once completed this form should be handed to the relevant Head of Year to be pre-assessed.
| For office use: Pre-assessment Date: ____________________ Signed: _______________________________________ OUTCOME: This referral is a: Tier 1 □ Tier 2 □ Tier 3 □ Tier 4 □ —————————————————————————————————————————————— Start: ____________________________ Finish: _________________________ No of sessions: _____________ |